
NURS FPX 8022 Assessment 1 Using Data to Make Evidence-Based Technology Recommendations
Student Name
Capella University
NURS-FPX8022 Nursing Technology and Advanced Healthcare Information Systems
Professor Name
Submission Date
Using Data to Make Evidence-Based Technology Recommendations
Evidence-based technology suggestions in healthcare settings are critical pillars of improving the quality of care and organizational performance in healthcare settings. By screening clinical studies, patient files, and operational data, the healthcare organizations are able to choose those technologies that are genuinely effective in enhancing service provision, and at the same time, they are cost-effective. The systematic implementation plan reduces operational risks and ensures that new technologies address real clinical issues and patient care problems rather than adopting technology trends without a purpose (Gentili et al., 2022). Information-based suggestions generate sustainable healthcare innovations that show quantifiable gains in patient outcomes and personnel procedures. The objective of the evaluation is to consider the use of technology in practice settings and utilize the performance data to develop evidence-based technology recommendations.
Evaluation of Technology in Use
Context
To deliver the best possible patient care and safety levels, healthcare organizations should conduct a systematic review of their performance outcomes in relation to the set of performance benchmarks on a national level. The Medical University of South Carolina University Medical Center (MUSC) exhibits significant gaps in performance with patient falls recorded at 0.792 and 0.000 in the best healthcare organizations, respectively, indicating that there is a need to improve patient safety urgently (Leapfrog, n.d.). The medication communication score of the institution is 76 out of 93 points, which is below the average of high-performing hospitals, and they score 93 points, which is a sign of the lack of patient education pertaining to prescribed treatment and side effects (Leapfrog, n.d.). The level of discharge communication is moderate with 84 points, which is slightly lower than the national average, but higher than the average of the low-rated facilities with 67 points (Leapfrog, n.d.). The implementation of strategic technology and training of the staff is essential in achieving excellence in the levels of patient safety and communication.
Benefits
The implementation of the interactive patient education systems and the use of automated medication delivery systems in the MUSC Medical Center significantly enhance the efficiency of medication communication and discharge plans. Precisely, the technologies will allow healthcare professionals to give consistent medication counseling and discharge education by means of touchscreen interfaces, including visual aids to make sure their patients have a complete understanding (Galmarini et al., 2024). Moreover, the systems eradicate changeable communication procedures and permit systematised records of patient understanding concerning medication administration and discharge guidelines (Mason et al., 2022). The standardized processes also lead to improved patient safety due to the presence of consistent medication and discharge communication processes, fostering improved treatment adherence. The overall strategy aims to fill the communication gaps that have been noticed in the performance measurement currently in the facility.
Obstacles to Utilizing Technology
Adoption of sophisticated communication technologies in healthcare organizations is a complex issue with organizational goals and human factors posing a major challenge. Among the key issues is the unwillingness of the staff to use interactive patient education platforms based on the fear of an extra workload and the inability to master digital interfaces, and to handle this issue, large-scale training programs are often necessary, which further strain the already limited resources (Schooley et al., 2020). The other significant issue revolves around the aspect of finances, since the price of acquiring automated medication delivery systems and staff to maintain the units is severely restricted due to budget constraints, especially for facilities with fewer staff. Moreover, technical integration issues also arise whereby connecting the new communication platforms to the existing electronic health record systems leads to serious disruption to the workflow. In addition, patients with low levels of digital literacy might not be able to use touchscreen-based systems of education effectively, which can result in the emergence of more health disparities, instead of fewer (Qin et al., 2024). As a result, thorough implementation plans and well-coordinated administrative reinforcement remain crucial in effective technology implementation at various healthcare facilities.
Workflow for the Usage of Chosen Technology
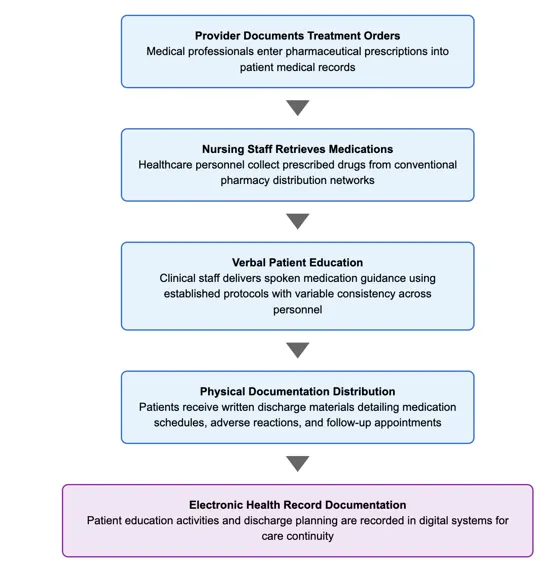
At the MUSC Medical Center, the existing medication communication and discharge system begins with providers entering medication orders into patient files, and then the nurses retrieve medications through customary pharmacy dispensing machines. Nurses give verbal medication education to patients with standardized protocols, but there is inconsistency across the staff. The workflow in the healthcare industry should maintain efficiency and maintain the overall patient knowledge and safety practice (Mistri et al., 2023). Communication strategies need structured plans that can support various learning needs and preferences of patients (Gessesse et al., 2023). The discharge instructions are given to the patients mostly through printed handouts informing them of their schedule of medication, side effects, and follow-up appointments. The system of documentation is carried out in the electronic health record system, and a lasting record of the patient education and discharge planning activities is recorded to facilitate continuity of care. This current system is shown in Appendix A.
Patient Safety Areas Identified
There are two major evaluation frameworks of healthcare facilities, such as Leapfrog Hospital Safety Grades and Medicare Care Compare. Namely, Leapfrog provides letter grades (A-D) in accordance with detailed safety measures, such as security measures against infections, medication safety, and patient outcomes data. Medicare Compare evaluates the different aspects of medical service delivery and patient satisfaction, which enables people to make comparative analyses when choosing healthcare providers (CMS, 2023). The assessment frameworks have three essential functions: enhancing transparency, promoting quality improvement, and providing consumers with evidence-based data to make informed choices of medical facilities (The Leapfrog Group, 2023). With the help of unified assessment standards, the monitoring frames mutually enhance healthcare standards by enabling informed decision-making processes.
The MUSC Medical Center’s Leapfrog Safety Grade
The health facility has significant patient safety and communication quality indicators across different performance domains. MUSC Medical Center in particular encounters difficulties with the prevention of patient falls, with a rate of 0.792, which is significantly higher than the benchmark institution with 0.000 and is much higher than industry rates with 0.384 (Leapfrog, n.d.). Medication communication (76) and discharge communication (84) demonstrate fairly good performance levels, but the values remain significantly lower as compared to the results of premier establishments of 93 and 97, respectively (Leapforg, n.d.). The rating creates doubts about the commitment of the medical center to comprehensive patient safety and educational excellence practices.
Table 1
Medical University of South Carolina University Medical Center Score Comparison
Categories | Facility Score | Top Facility Score | Average Facility’s Score | Lowest Center’s Score |
Patient Falls and Injuries | 0.792 | 0.000 | 0.384 | 1.926 |
Medication Communication | 76 | 93 | 74.42 | 55 |
Discharge Communication | 84 | 97 | 85.25 | 67 |
Note. Information gives Leapfrog safety grade scores of the Medical University of South Carolina University Medical Center in comparison with the industry standard scores. Lower scores would indicate high performance in terms of patient falls measurements, and higher scores indicate high performance in terms of communication measurements. Data were accessed through the database of Leapfrog Hospital Safety Grade (Leapfrog, n.d).
Medicare Compare Score
The MUSC Medical Center has inconsistent Medicare quality performance in several healthcare measures. The facility has a 4-star rating in terms of overall star rating and a 4-star rating in terms of patient survey (Medicare, n.d.). The medical center also does well in follow-up guidance in colonoscopy, at 98% versus the national average of 92, stroke treatment, with 81% receiving brain imaging within 45 minutes compared to 70% national level, and the emergency department performance, where 53% versus 63% of the national standard is problematic (Medicare, n.d.). The institution shows great compliance with flu vaccinations, at 90 percent versus the national 80 percent, as well as superiority in a number of infection control indicators, such as central line-related bloodstream infection and catheter-related urinary tract infection (Medicare, n.d.). There are significant delays in emergency department operations, with a 222-minute average length of stay versus a 194-minute average length of stay in other high-volume hospitals in the country, and 5% of patients leaving without treatment as opposed to the national 2-percent (Medicare, n.d.). The results point to the need to make improvements in emergency department processes and sepsis identification procedures in health care delivery models.
Comparative Hospital Analysis
The healthcare performance metrics reveal significant differences in operations across leading academic healthcare facilities in diverse service lines. Cleveland Clinic also develops some gaps in medication communication at 58% compared to Mayo Clinic Jacksonville at 66, and both facilities have troubles with sepsis management lower than the national level of 63 and 64, respectively (Medicare, 2025a; Medicare, 2025b). The Cleveland Clinic had an alarming 189 minutes waiting time, compared to Mayo Clinic Jacksonville, with a long wait time of 202 mins with a patient exit percentage of 6 and 1 before assessment, as per the emergency department effectiveness was alarming. The adherence levels of influenza immunization show amazing disparities between the 90% level of the Cleveland Clinic and the poor 69% level of the Mayo Clinic Jacksonville in comparison with the national level of 80% (Medicare, 2025a; Medicare, 2025b). The proportions of Medicare expenditure show financial management deviations at 0.94 and 0.99, respectively, as compared with the national 0.99 mean, and the infection control demonstrates better results during the management of catheter-related urinary tract infections and central line-associated bloodstream infection (Medicare, 2025a; Medicare, 2025b). The Cleveland Clinic and Mayo Clinic Jacksonville both achieve better mortality outcomes with cardiac conditions and pneumonia than the national performance rates, with the Cleveland Clinic having 9.8% heart attack mortality, and Mayo Clinic Jacksonville having 9% heart failure mortality. One of the most crucial elements of maximizing patient care and operational efficiency in any large healthcare organization remains systematic quality enhancement programs.
Recommended Technology Implementation
To address the existing performance deficiencies, the MUSC Medical Center ought to introduce the use of a system of bedside interactive patient education tablets equipped with automated medication dispensing devices. A study indicated that healthcare facilities implementing the built-in technologies realized significant changes in medication errors as well as patient understanding measurements during deployment times (Murthi et al., 2024). The interactive patient education system has to be integrated with personalized multimedia-based information, multilingual support features, and the ability to document and retrieve information in real time to seal considerable performance gaps among various quality indicators. In particular, the current scores of medication communication of the organization are 76 points compared to industry leaders that have 93 points, patient falls of 0.792 incidents per 1,000 patient days are higher than the best-ranked hospitals with 0.000 incidents, and the discharge communication score is 84 points, which is lower than the best institutions with 97 points, which is a critical area of Also, the use of automated patient response collection through touchscreen technology might enhance the quality assessment procedures, which may also improve the overall patient satisfaction rating (Leonardsen et al., 2020). The combined technological strategy entails the utilization of existing electronic medical record systems and aims at addressing specific flaws in patient communication procedures and safety measures throughout the healthcare delivery spectrum.
Improvement After Redesign
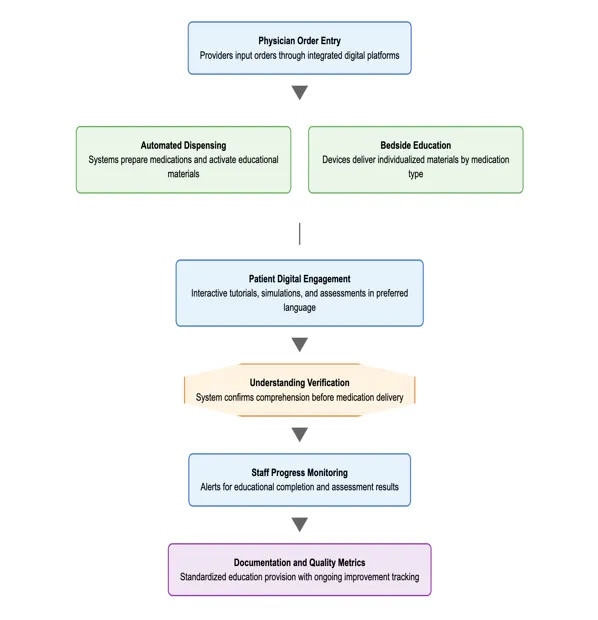
The medication management protocol after integrating technology becomes an interactive digital workflow involving patients during treatment episodes instead of traditional verbal communications. To begin with, the work of a physician in ordering medications is processed and documented using a set of computerized platforms, which offer the basis of automated care coordination. Second, automated dispensing machines prepare drugs and activate patient bedside educational resources in response to certain drug properties at the same time (Tu et al., 2023). Third, the digital interface will offer patients customized video tutorials, simulations, which are practical and knowledge assessments in their favored language, and can best understand. Next, the automated alerts on the completion and comprehension tests of educational modules alert clinical staff to the further advancement of patients and launch medicine administration procedures (Elbeddini and Tayefehchamani, 2021). Lastly, the safety measures include absolute completion of the educational stages prior to pharmaceutical dispensing and a requirement to establish that the patients have acquired the skills of proper administration methods and possible side effects (Manias et al., 2020). The streamlined process eliminates information obstacles, standardizes the delivery of patient education, and develops measures of continuous quality improvement. The improved workflow is presented in Appendix B.
Conclusion
The use of evidence-based technology is a fundamental approach that medical institutions aiming to achieve sustainable improvement in their clinical outcomes and institutional performance take. The research shows that automated pharmaceutical dispensing systems, together with the digital patient education systems, significantly enhance the medication safety procedures and communication. By using the insights of thorough quality measures of Leapfrog and Medicare comparison repositories, healthcare facilities will be able to identify shortcomings systematically and implement targeted technological interventions. The strategy enables hospitals to address specific areas of weakness and achieve measurable quality improvements in care provision levels and patient satisfaction metrics.
Step By Step Instructions To Write
NURS FPX 8022 Assessment 1
Contact us to receive step-by-step instructions.
Instruction file for
NURS FPX 8022 Assessment 1
Contact us to get the instruction file.
Scoring Guide for
NURS FPX 8022 Assessment 1
Contact us to get the Scoring file.
References For
NURS FPX 8022 Assessment 1
CMS. (2023, September 6). Hospital quality initiative public reporting | CMS. Cms.gov. https://www.cms.gov/medicare/quality/initiatives/hospital-quality-initiative/hospital-compare
Elbeddini, A., & Tayefehchamani, Y. (2021). Development and evaluation of an online medication safety module for medical students at a rural teaching hospital: The Winchester District Memorial Hospital. BioMed Journal Open Quality, 10(2), e001385. https://doi.org/10.1136/bmjoq-2021-001385
Galmarini, E., Marciano, L., & Schulz, P. J. (2024). The effectiveness of visual-based interventions on health literacy in health care: A systematic review and meta-analysis. BioMed Central Health Services Research, 24(1), 1–10. https://doi.org/10.1186/s12913-024-11138-1
Gentili, A., Failla, G., Melnyk, A., Puleo, V., Tanna, G. L. D., Ricciardi, W., & Cascini, F. (2022). The cost-effectiveness of digital health interventions: A systematic review of the literature. Frontiers in Public Health, 10(10), e787135. https://doi.org/10.3389/fpubh.2022.787135
Gessesse, A. G., Haile, J. M., & Woldearegay, A. G. (2023). Exploring effective communication strategies employed by physicians in delivering bad news in Ethiopian state hospitals. Patient Related Outcome Measures, 14, 409–425. https://doi.org/10.2147/PROM.S390164
Leapforg. (n.d.). Medical University of South Carolina University Medical Center – SC – Hospital Safety Grade. Hospitalsafetygrade.org. https://www.hospitalsafetygrade.org/h/medical-university-of-south-carolina-university-medical-center
Leonardsen, A.-C. L., Hardeland, C., Helgesen, A. K., & Grøndahl, V. A. (2020). Patient experiences with technology enabled care across healthcare settings- A systematic review. BioMed Central Health Services Research, 20(1), 779. https://doi.org/10.1186/s12913-020-05633-4
Mason, M., Cho, Y., Rayo, J., Gong, Y., Harris, M., & Jiang, Y. (2022). Technologies for medication adherence monitoring and technology assessment criteria: Narrative review. Journal of Medical Internet Research MHealth and UHealth, 10(3), e35157. https://doi.org/10.2196/35157
Medicare. (2025a). Find healthcare providers: Compare care near you | Medicare. Medicare.gov. https://www.medicare.gov/care-compare/details/hospital/100151/view-all?city=Jacksonville&state=FL&zipcode=&measure=hospital-timely-and-effective-care
Medicare. (2025b). Find healthcare providers: Compare care near you | Medicare. Medicare.gov. https://www.medicare.gov/care-compare/details/hospital/360180/view-all?city=Cleveland&state=OH&zipcode=&measure=hospital-timely-and-effective-care
Medicare. (n.d.). Find healthcare providers: Compare care near you | Medicare. Medicare.gov. https://www.medicare.gov/care-compare/details/hospital/420004/view-all?city=Charleston&state=SC&zipcode=29425
Mistri, I. U., Badge, A., & Shahu, S. (2023). Enhancing patient safety culture in hospitals. Cureus, 15(12), 1–7. https://doi.org/10.7759/cureus.51159
Murthi, S., Martini, N., Falconer, N., & Scahill, S. (2024). Evaluating ehr-integrated digital technologies for medication-related outcomes and health equity in hospitalised adults: A scoping review. Journal of Medical Systems, 48(1), 1–19. https://doi.org/10.1007/s10916-024-02097-5
Qin, C., Zhu, Y., Li, D., & Liu, C. (2024). The impact of digital skills on health: Evidence from the China General Social Survey. Digital Health, 10. https://doi.org/10.1177/20552076241304592
Schooley, B., Singh, A., Hikmet, N., Brookshire, R., & Patel, N. (2020). Integrated digital patient education at the bedside for patients with chronic conditions: Observational study. Journal of Medical Internet Research MHealth and UHealth, 8(12), e22947. https://doi.org/10.2196/22947
The Leapfrog Group. (2023, November 3). New hospital safety grades from The Leapfrog Group find improved infection rates following major spike during the COVID-19 pandemic. Leapfrog.org. https://www.leapfroggroup.org/news-events/new-hospital-safety-grades-leapfrog-group-find-improved-infection-rates-following-major
Tu, H. N., Shan, T. H., Wu, Y. C., Shen, P. H., Wu, T. Y., Lin, W. L., Kao, Y. H. Y., & Cheng, C. L. (2023). Reducing medication errors by adopting automatic dispensing cabinets in critical care units. Journal of Medical Systems, 47(1), 52. https://doi.org/10.1007/s10916-023-01953-0
Appendix for
NURS FPX 8022 Assessment 1
Appendix A: Current Medication Communication and Discharge Workflow
Appendix B: Redesigned Workflow with Interactive Patient Education Systems and Automated Medication Dispensing
Capella Professors To Choose From For NURS-FPX8022 Class
- Jacqueline McCoy.
- Jessica Mioduszewski.
(FAQs) related to
NURS FPX 8022 Assessment 1
Question 1: What is NURS FPX 8022 Assessment 1 Using Data to Make Evidence-Based Technology Recommendations?
Answer 1: Using healthcare data to evaluate and recommend evidence-based technology solutions.
Do you need a tutor to help with this paper for you within 24 hours
- 0% Plagiarised
- 0% AI
- Distinguish grades guarantee
- 24 hour delivery
Next Assessment: