
Student Name
Capella University
MHA-FPX5020 Health Administration Capstone
Instructor Name
Submission Date
PROBLEM STATEMENT
Medication errors can happen due to a lack of protocol and poor communication during a handoff of patients between healthcare providers. Medication errors can lead to adverse drug reactions, longer stays in a hospital, more money spent on healthcare, harm to the patients, and death (Agency for Healthcare Research and Quality, 2023; The Joint Commission, 2025).
FACTORS AND METRICS
Path 2:
Factor #1 Examined | Medication Reconciliation Accuracy at Patient Admission |
Precise Unit of Measurement (days, dollars, %…) | % of patients with unintended medication discrepancies (UMD) |
Type of Graphic Data Summary (pie chart, bar graph, other) | Bar graph showing percentage of patients with and without medication discrepancies at admission |
Source of Data (APA Format) | Moges, T. A., Akalu, T. Y., & Sema, F. D. (2022). Unintended medication discrepancies and associated factors upon patient admission to the internal medicine wards: Identified through medication reconciliation. BioMed Central Health Services Research, 22(1), e1090. https://doi.org/10.1186/s12913-022-08628-5 |
Factor #2 Examined | Types of Medication Discrepancies During Care Transitions |
Precise Unit of Measurement (days, dollars, %…) | % distribution by type of discrepancy |
Type of Graphic Data Summary (pie chart, bar graph, other) | Pie chart showing breakdown of medication discrepancy types |
Source of Data (APA Format) | Moges, T. A., Akalu, T. Y., & Sema, F. D. (2022). Unintended medication discrepancies and associated factors upon patient admission to the internal medicine wards: Identified through medication reconciliation. BioMed Central Health Services Research, 22(1), e1090. https://doi.org/10.1186/s12913-022-08628-5 |
Factor #3 Examined | Impact of Pharmacist-Led Medication Reconciliation on Error Reduction |
Precise Unit of Measurement (days, dollars, %…) | Number of medication discrepancies identified |
Type of Graphic Data Summary (pie chart, bar graph, other) | Comparative bar graph |
Source of Data (APA Format) | Hammour, K. A., Farha, R. A., Ya’acoub, R., Salman, Z., & Basheti, I. (2022). Impact of pharmacist-directed medication reconciliation in reducing medication discrepancies: A randomized controlled trial. Canadian Journal of Hospital Pharmacy, 75(3), 191–199. https://doi.org/10.4212/cjhp.3143 |
Factor #1 Graphic Structure
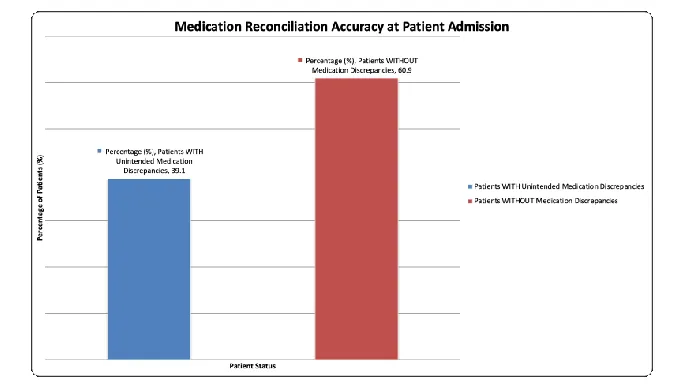
Medication Reconciliation Accuracy at Patient Admission, Ethiopian Hospitals (Felege Hiwot & Tibebe Ghion), 2021
Moges, T. A., Akalu, T. Y., & Sema, F. D. (2022). Unintended medication discrepancies and associated factors upon patient admission to the internal medicine wards: Identified through medication reconciliation. BioMed Central Health Services Research, 22(1), e1090. https://doi.org/10.1186/s12913-022-08628-5
Factor 1 Graphic Observation or Insight |
A. Over one third (39.1) of wards of internal medicine had one or more unintended medication discrepancies, which is reported to be a high patient safety issue at the hospital admission point, which is directly related to medication errors and adverse drug events. |
B. The medication discrepancies are 248 patients out of 635 hospital admissions, reflecting a high volume of problems and potentially leading to the emergence of long-stay hospitalizations, increased healthcare costs, and preventable injuries to patients if the problem is not solved. |
C. The majority of patients (60.9) underwent the correct medication reconciliation, which demonstrated that though these errors frequently occur, the correct measures and steps can be taken to reduce the discrepancies, and that therefore the standard protocol should be used routinely with every patient admitted. |
Factor #2 Graphic Structure
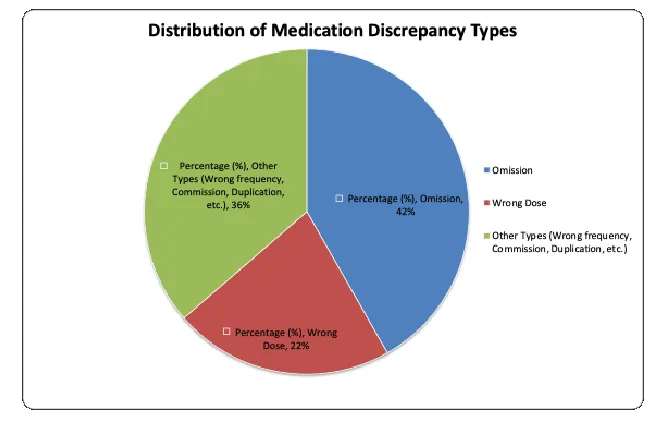
Types of Medication Discrepancies During Care Transitions, Ethiopian Hospitals (Felege Hiwot & Tibebe Ghion), 2021
Moges, T. A., Akalu, T. Y., & Sema, F. D. (2022). Unintended medication discrepancies and associated factors upon patient admission to the internal medicine wards: Identified through medication reconciliation. BioMed Central Health Services Research, 22(1), e1090. https://doi.org/10.1186/s12913-022-08628-5
Factor 2 Graphic Observation or Insight |
A. Omission (41.75% – 162 pieces of medication) was the most common type of medication discrepancy, which means that medicines previously given to the patient were not continued upon hospital admission. |
B. The overall omission and wrong dose errors prevalence (63.65) shows that the two types of mistakes comprise almost two-thirds of all medication errors. |
C. The rest of the 36.35 percent (141 medications) of discrepancies involve a variety of types of errors, such as the incorrect frequency, commission, and duplication. |
FACTOR #3 GRAPHIC STRUCTURE
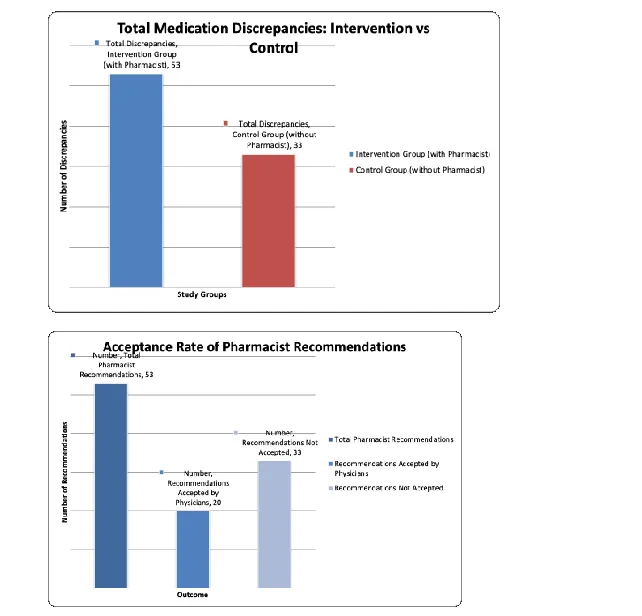
Impact of Pharmacist-Led Medication Reconciliation on Error Reduction, Jordan University Hospital Surgical Wards, 2017-2018
Hammour, K. A., Farha, R. A., Ya’acoub, R., Salman, Z., & Basheti, I. (2022). Impact of pharmacist-directed medication reconciliation in reducing medication discrepancies: A randomized controlled trial. Canadian Journal of Hospital Pharmacy, 75(3), 191–199. https://doi.org/10.4212/cjhp.3143
Construct a data summary graphic and insert it below. Make sure that all axes or sections are clear.
Factor 3 Graphic Observation or Insight |
A. There were significantly more medication discrepancies found in the intervention group (53/61 patients) versus the control group (33/62 patients), where the medication reconciliation was led by the pharmacists. |
B. 20 percent of the accepted recommendations effectively resolved medication discrepancies, although 38 percent of the pharmacists’ recommendations were accepted by the treating doctors. |
C. Statistically significant reductions in all types of medication discrepancies were found upon admission and discharge in both intervention and control groups (p = 0.002 and p = 0.007, respectively). |
D. The randomized controlled trial study offers good evidence that medication reconciliation services directed by pharmacists in the surgical wards can be effective in alleviating accidental medication discrepancies. |
EVIDENCE-BASED RECOMMENDATIONS
Recommendation: | Source |
1. Introduce pharmacist-directed medication reconciliation during hospital admission with a priority to high-risk patients such as patients aged 65 years and above, patients on polypharmacy (at least 5 medications), and patients with various comorbidities. | Moges, T. A., Akalu, T. Y., & Sema, F. D. (2022). Unintended medication discrepancies and associated factors upon patient admission to the internal medicine wards: Identified through medication reconciliation. BioMed Central Health Services Research, 22(1), e1090. https://doi.org/10.1186/s12913-022-08628-5 |
2. Implement a procedure for the healthcare teams to obtain a medication history from at least two sources (patient, family member, medical record, and/or medication bottles) to improve the accuracy of medication reconciliation. | Moges, T. A., Akalu, T. Y., & Sema, F. D. (2022). Unintended medication discrepancies and associated factors upon patient admission to the internal medicine wards: Identified through medication reconciliation. BioMed Central Health Services Research, 22(1), e1090. https://doi.org/10.1186/s12913-022-08628-5 |
3. Now start to introduce clinical pharmacists to surgical ward teams in order to deliver medication reconciliation services and make evidence-based recommendations to physicians to try to resolve discrepancies of medications that need to be either initiated or de-escalated at the care transition phase. | Hammour, K. A., Farha, R. A., Ya’acoub, R., Salman, Z., & Basheti, I. (2022). Impact of pharmacist-directed medication reconciliation in reducing medication discrepancies: A randomized controlled trial. Canadian Journal of Hospital Pharmacy, 75(3), 191–199. https://doi.org/10.4212/cjhp.3143 |
4. Develop and implement standardized policies, procedures, and guidelines for clinical practice on interprofessional medication reconciliation at discharge and make clear the roles and responsibilities of the nurse, pharmacist, and physician in the hospital setting. | Latimer, S., Hewitt, J., de Wet, C., Teasdale, T., & Gillespie, B. M. (2022). Medication reconciliation at hospital discharge: A qualitative exploration of acute care nurses’ perceptions of their roles and responsibilities. Journal of Clinical Nursing, 32(7-8), 1276–1285. https://doi.org/10.1111/jocn.16275 |
5. Introduce mandatory specialized training to all nursing personnel on the process of medication reconciliation, recognizing medication discrepancies, ways to educate patients, and documentation roles. | Latimer, S., Hewitt, J., de Wet, C., Teasdale, T., & Gillespie, B. M. (2022). Medication reconciliation at hospital discharge: A qualitative exploration of acute care nurses’ perceptions of their roles and responsibilities. Journal of Clinical Nursing, 32(7-8), 1276–1285. https://doi.org/10.1111/jocn.16275 |